
October 12, 2023
By: Danruo Zhong, Bonny Donzella, and Megan Gunnar
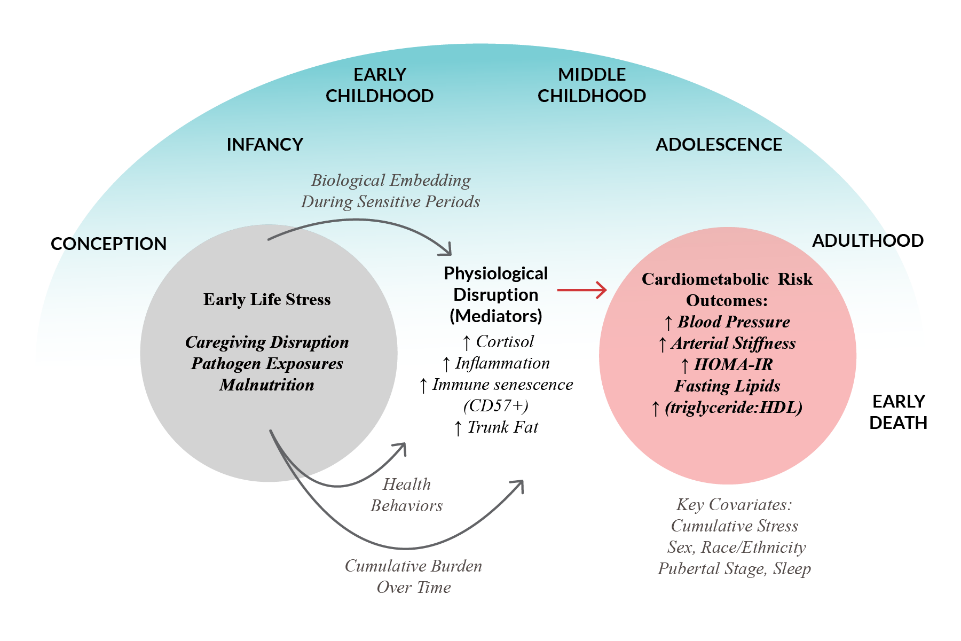
Recently, the American Heart Association concluded that adult cardiometabolic disease can be traced, in some instances, to early life stress (ELS) conditions. They also noted the need to determine sensitive periods during which exposure to adversity alters systems contributing to cardiometabolic risk and thus when interventions will be the most effective.
These are the goals of the CardioHealth Study. By comparing youth adopted into well-resourced families from conditions of relative deprivation and adversity early in life to youth who were born into and raised in similarly well-resourced families, we are examining the question of whether very early experiences present an increase in risk for poor heart health that we can detect as early as adolescence. Thus, for two years, with the help of families like yours, we enrolled more than 190 youth aged 12-22 into our study, with about half of the sample made up of youth who were adopted internationally from orphanage-like care (hereafter, PI for previously institutionalized) and half were non-adopted (NA) having been born into their families in Minnesota. The first wave of data collection was completed in February 2023, the assays have been run, and we are now beginning to analyze those data.
Generally speaking, both PI and NA youth are more fit than the average youth in the US. This is not surprising as cardiometabolic health is correlated with social class and both PI and NA youth have typically lived in relatively well-educated and higher income families the majority of their lives. One example is body mass index (BMI). The 85th percentile is the cutoff for overweight, and the 95th for obese. The Center for Disease Control estimates that 22% of the adolescent population in the US suffers from obesity. In our sample, the percentage was about half that or 12%. Among the NA youth, we had even fewer, 8%, in the obese range, while we did see some evidence of increased risk for PI youth (16%, with the risk carried by the male PI youth, 27%).
Allostatic Load
One way of examining the impact of early life adversity is to calculate something called “allostatic load.” Allostasis is the idea that when we are threatened (psychologically or physically) we mount stress responses that include elevated cortisol, adrenaline, and immune (inflammation) responses. Allostasis means achieving stability through change and the idea is that by mounting these stress responses we are stabilizing ourselves and allowing ourselves to cope with the immediate threat. This is good. But there is a cost. When we mount these responses relatively infrequently, the costs are minimal. But when we need to do this a lot, costs are greater, and we begin to see alterations in systems impacted by stress. Allostatic load is a summing up of the systems that show the impact of chronic stress activation.
In orphanages or orphanage-like institutions, children receive little individual care. They are often exposed to viruses and other pathogens, and they fall behind in physical and behavioral milestones. Once they are adopted, they often show remarkable rebounds. Yet, those few orphanage years may result in evidence of greater allostatic load years later. Thus, as a first pass through our data, we used the first assessments for each participant to calculate a measure of allostatic load. The cardiometabolic system is a major target of stress and thus measures of cardiometabolic health are typically used to calculate Allostatic Load.
We used the following measures to calculate allostatic load: [Note that if any measure was in a clinical range, we have already contacted the family. The means of these measures are in “normal” range, even when one group has a higher mean level than the other.]
- Hair Cortisol: Cortisol is a necessary hormone even when we are not stressed. Cortisol increases with stress and both stress and basal cortisol levels accumulate in hair. We took hair samples that gave us a calendar of cortisol produced in the last 3 months.
- C-Reactive Protein: This can be considered a cumulative measure of inflammation.
- IL-6: This is a cytokine that works in the immune system to trigger an immune response. It is also an index of inflammatory activity.
- TNF-alpha: Another cytokine that is important in inflammation.
- Insulin: Insulin moves sugar out of the blood system and into storage.
- HDL and LDL cholesterol: “Good vs bad” cholesterol.
- Triglycerides: The most common lipid in circulation.
- Plasma Glucose Level: The level of sugar present in blood.
- Systolic and Diastolic Blood Pressure: The pressure of blood in the circulatory sytem.
- Waist-hip ratio and Body Mass Index: Higher waist-hip ratio is a risk for cardiometabolic disease and higher body mass (weight for height) is also a risk factor.
To calculate allostatic load, we gave participants a score of 1 for every one of their measures that was in the top 25% in whatever range (high or low) is evidence of chronic stress activation.
What did we learn when we combined all the measures and summed the number of scores for each participant?
1.) Males tend to have higher allostastic load (AL) scores than females (here we used sex assigned at birth), 2) with age, allostatic load scores increased (our participants ranged from 12-22 years), 3) higher current life stress calculated from an online self-report was associated with higher AL scores. But independent of all these effects, PI youth had higher AL scores than NA youth. The difference was an average of 3.6 for the PI youth and 2.7 for the NA youth. Keep in mind that the score was out of 12, so both groups are still carrying a relatively light load.
Conclusions: We have a lot of data yet to analyze from the first assessment. We are now seeing the youth for a second assessment to see if changes in AL and in other measures of cardiometabolic risk change more rapidly during the adolescent or young adult years for one group or the other. We also expect that the extent to which the PI youth were delayed in their physical growth at the time of adoption may be a critical measure in identifying those youth with higher risk. We are contacting families where we are missing this information to be sure we have information on this from all PI participants.
The bottom line for participants: Some of our participants, especially those with early histories of institutional care, will need to be vigilant about diet, exercise and tracking their heart health as they age.
The bottom line for policy makers: a) Orphanages are not the best places to raise babies. Dr. Gunnar along with other researchers who study the effects of institutions around the world are advocating for finding more family-like ways of dealing with the many children worldwide who are without permanent parents. b) As we think about how early we need to intervene to support families and children in the US as well as worldwide, we need to think very early. In the womb and the first few years are critical years that have effects on life-long health. Dr. Gunnar is working with researchers throughout the US and in Minnesota to advocate for family-friendly policies. For many years she has been on the advisory committee to the Governor of Minnesota’s Children’s Cabinet and she was a founding member of the National Scientific Council on the Developing Child that works to translate research on child development for the use of policy makers and practitioners.
Stay tuned! The second wave of collection is underway! We are reaching out to families to schedule their follow-up visits. If you have already participated, watch for an email from cariodhealth@umn.edu or a text from our study phone (612) 492-1253. We will contact you a month or two before the second anniversary of your participation.